Search for drugs:
Typing the drug name to query
FLECAINIDE ACETATE
DIR Classification
Classification:Most-DIQT concern
Severity Score:4.0
Description in Drug Labeling: View Full Labeling: SPL in DailyMed | PDF
- WARNINGS
- HEART FAILURE
- Flecainide has a negative inotropic effect and may cause or worsen CHF, particularly in patients with cardiomyopathy, preexisting severe heart failure (NYHA functional class III or IV) or low ejection fractions (less than 30%). In patients with supraventricular arrhythmias new or worsened CHF developed in 0.4% (1/225) of patients. In patients with sustained ventricular tachycardia, during a mean duration of 7.9 months of flecainide therapy, 6.3% (20/317) developed new CHF. In patients with sustained ventricular tachycardia and a history of CHF, during a mean duration of 5.4 months of flecainide therapy, 25.7% (78/304) developed worsened CHF. Exacerbation of preexisting CHF occurred more commonly in studies which included patients with class III or IV failure than in studies which excluded such patients. Flecainide should be used cautiously in patients who are known to have a history of CHF or myocardial dysfunction. The initial dosage in such patients should be no more than 100 mg bid (see DOSAGE AND ADMINISTRATION) and patients should be monitored carefully. Close attention must be given to maintenance of cardiac function, including optimization of digitalis, diuretic, or other therapy. In cases where CHF has developed or worsened during treatment with flecainide, the time of onset has ranged from a few hours to several months after starting therapy. Some patients who develop evidence of reduced myocardial function while on flecainide can continue on flecainide with adjustment of digitalis or diuretics, others may require dosage reduction or discontinuation of flecainide. When feasible, it is recommended that plasma flecainide levels be monitored. Attempts should be made to keep trough plasma levels below 0.7 to 1.0 mcg/mL.
- Effects on Cardiac Conduction
- Flecainide slows cardiac conduction in most patients to produce dose-related increases in PR, QRS, and QT intervals. PR interval increases on average about 25% (0.04 seconds) and as much as 118% in some patients. Approximately one-third of patients may develop new first-degree AV heart block (PR interval ≥ 0.20 seconds). The QRS complex increases on average about 25% (0.02 seconds) and as much as 150% in some patients. Many patients develop QRS complexes with a duration of 0.12 seconds or more. In one study, 4% of patients developed new bundle branch block while on flecainide. The degree of lengthening of PR and QRS intervals does not predict either efficacy or the development of cardiac adverse effects. In clinical trials, it was unusual for PR intervals to increase to 0.30 seconds or more, or for QRS intervals to increase to 0.18 seconds or more. Thus, caution should be used when such intervals occur, and dose reductions may be considered. The QT interval widens about 8%, but most of this widening (about 60% to 90%) is due to widening of the QRS duration. The JT interval (QT minus QRS) only widens about 4% on the average. Significant JT prolongation occurs in less than 2% of patients. There have been rare cases of Torsade de Pointes-type arrhythmia associated with flecainide therapy.
- Clinically significant conduction changes have been observed at these rates: sinus node dysfunction such as sinus pause, sinus arrest and symptomatic bradycardia (1.2%), second degree AV block (0.5%) and third-degree AV block (0.4%). An attempt should be made to manage the patient on the lowest effective dose in an effort to minimize these effects. (See DOSAGE AND ADMINISTRATION.) If second- or third-degree AV block, or right bundle branch block associated with a left hemiblock occur, flecainide therapy should be discontinued unless a temporary or implanted ventricular pacemaker is in place to ensure an adequate ventricular rate.
- OVERDOSAGE
- No specific antidote has been identified for the treatment of flecainide overdosage. Overdoses ranging up to 8000 mg have been survived, with peak plasma flecainide concentrations as high as 5.3 mcg/mL. Untoward effects in these cases included nausea and vomiting, convulsions, hypotension, bradycardia, syncope, extreme widening of the QRS complex, widening of the QT interval, widening of the PR interval, ventricular tachycardia, AV nodal block, asystole, bundle branch block, cardiac failure, and cardiac arrest. The spectrum of events observed in fatal cases was much the same as that seen in the non-fatal cases. Death has resulted following ingestion of as little as 1000 mg; concomitant overdose of other drugs and/or alcohol in many instances undoubtedly contributed to the fatal outcome. Treatment of overdosage should be supportive and may include the following: removal of unabsorbed drug from the gastrointestinal tract, administration of inotropic agents or cardiac stimulants such as dopamine, dobutamine or isoproterenol; mechanically assisted respiration; circulatory assists such as intra-aortic balloon pumping; and transvenous pacing in the event of conduction block. Because of the long plasma half-life of flecainide (12 to 27 hours in patients receiving usual doses), and the possibility of markedly non-linear elimination kinetics at very high doses, these supportive treatments may need to be continued for extended periods of time.
- Hemodialysis is not an effective means of removing flecainide from the body. Since flecainide elimination is much slower when urine is very alkaline (pH 8 or higher), theoretically, acidification of urine to promote drug excretion may be beneficial in overdose cases with very alkaline urine. There is no evidence that acidification from normal urinary pH increases excretion.
Postmarketing Surveillance
Contingency Table:
Current Drug
Other Drugs
QT Prolongation
89
24003
Other ADRs
5982
38375605
Odds Ratio = 23.787
Drug Property Information
ATC Code(s):
- C01BC04 - flecainide acetate
- C01BC - "Antiarrhythmics, class Ic"
- C01B - "ANTIARRHYTHMICS, CLASS I AND III"
- C01 - CARDIAC THERAPY
- C - CARDIOVASCULAR SYSTEM
Active Ingredient:FLECAINIDE ACETATE
Active Ingredient UNII:M8U465Q1WQ
Drugbank ID:DB01195
PubChem Compound:3356
CTD ID:D005424
PharmGKB:PA449646
CAS Number:54143-55-4
Dosage Form(s):tablet
Route(s) Of Administrator:oral
Daily Dose:
- 200.0 mg/day C01BC04
Chemical Structure: 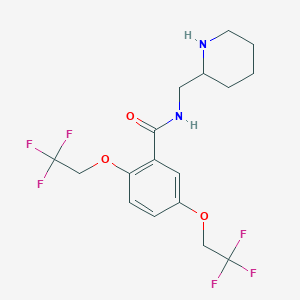
SMILE Code:
FC(F)(F)COC1=CC(C(=O)NCC2CCCCN2)=C(OCC(F)(F)F)C=C1
FC(F)(F)COC1=CC(C(=O)NCC2CCCCN2)=C(OCC(F)(F)F)C=C1
Reference
1: [QT prolongation and induction of torsades de pointe by flecainide. Apropos of a case].
[Wickers F,Haissaguere M,Palussiere J]Arch Mal Coeur Vaiss,1988 Oct;81(10):1283-5. PMID: 3146965
2: Flecainide: its proarrhythmic effect and expected changes on the surface electrocardiogram.
[Morganroth J,Horowitz L N]Am J Cardiol,1984 Feb 27;53(5):89B-94B. PMID: 6695821
Disclaimer:
The content of this database of QT prolongation is intended for educational and scientific research purposes only. It is not intended as a substitute for professional medical advice, diagnosis or treatment.
Any mention of commercial products is for clarification and not intended as endorsement.